Strength in Numbers #88
I had dinner with a friend of mine who is a great physical therapist a few nights ago and said something to the effect of,
“If you want to stay current, conduct research. If you want to be informed, read research within the past two years. If you want to be outdated, read textbooks.”
It resonated with me as what has been published in textbooks is still practiced in sports performance today and is taken at gospel value despite current evidence that tells us to go in a different direction.
STOP THE INSANITY
In the past, I have communicated about the dangers of focusing on passive range of motion as the most important assessment for injury prediction.
This is based on my experience in professional baseball, with over 450 pitchers. However, despite writing about this, we are still asked how our technology stands up to this old “gold standard” of passive range of motion.
But my prayers were answered when a scientific journal article surfaced in my publication notices only a week ago, and now I am convinced it is not the gold standard that can be sustained in the real world, as our athletes are not around clinical providers every day to catch a change in range of motion.
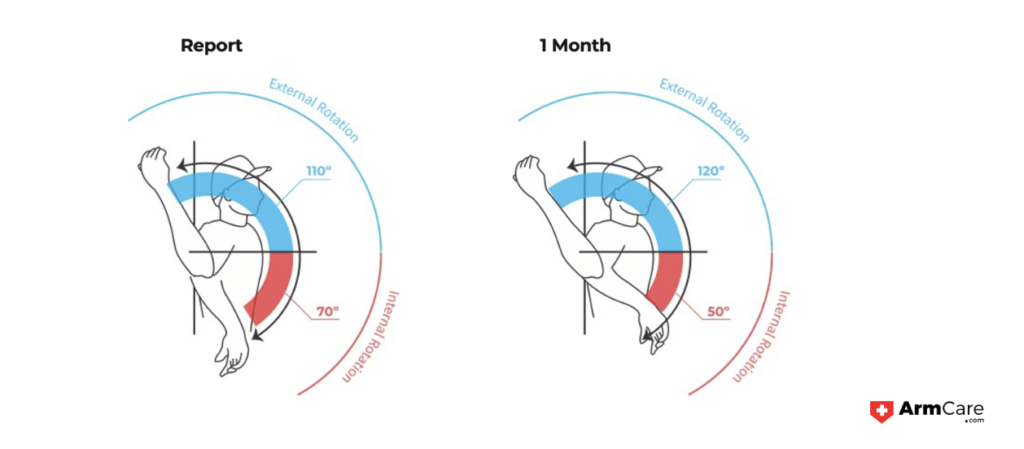
For those of you who may not know what goniometry means, it’s essentially a clinical tool that works like a 360-degree compass or protractor you would use in grade school.
You put the center of the goniometer at the approximate location or landmark for the center of the joint you want to measure, being the axis of rotation. Then the movable arm follows the segment to record a range of motion about a joint.
For the shoulder, the goniometer is aligned with the elbow and follows the forearm when it moves.
Tests are done supine, meaning belly up, lying down, and the arm starts perpendicular to the ground. Generally, clinicians are examining if a player can get their arm past 90 degrees or rotate below the plane of the table, indicating what is considered an “adequate range of motion” in external rotation and more than 25 degrees in internal rotation of the shoulder with the palm moving toward the table.

CRANKING BACK THE CATAPULT
The eureka moment for me concerning the highlighted scientific article was their statement indicating that passive range of motion assessment at the shoulder offers a limited predictive value of determining future UCL injuries—the true epidemic we are facing at all levels of play.
What has emerged now is that the component range of motion values (external rotation and internal rotation), in a passive sense, does not matter as much in injury prevention.
Essentially the new research criteria aimed to prevent TJ surgery indicate that athletes should have a similar total arc between limbs (ER+IR Range of Motion) and that there should be a surplus of external rotation (greater external rotation of at least 5 degrees) on the throwing arm versus the non-throwing arm.
However, the mixed view of the total arc versus looking at the component range of motion causes major problems, and I will explain why.
I have seen athletes come into Spring Training who have the same total arc but lack external rotation for the throwing arm in relation to the non-throwing arm. The typical first approach with the athlete has been to hyper-mobilize athletes’ arms into external rotation to create an external rotation surplus.
This increase in external rotation could contribute to greater throwing velocity, but it also increases instability! And instability is considered the major injury dart thrown into a baseball player’s elbow during a velocity enhancement program.
COMMIT THIS TO MEMORY – YOU WANT A STRONG AND LONG MUSCLE, BUT LENGTH WITHOUT STRENGTH IS THE KISS OF DEATH.
In baseball physical therapy, it’s shown that most experienced physical therapists representing Major League Staff are preoccupied with passive range of motion over strength or pain as readiness assessments. And on top of that, they may be intervening almost exclusively from this initial orthopedic evaluation (the paper can be downloaded here).
An aggressive approach to the first orthopedic measurements is not the best approach in my mind early in Spring Training as a few things happen over the course of time in camp.
- For starters, the collagen in the throwing arm starts to lay more evenly with higher-intensity throwing. These changes occur because the stabilizers are stretched with throwing, plus the warmer weather helps improve compliance for the muscles, tendons, and ligaments around the shoulder and elbow.
- Another occurrence is that the elbow’s ulnar collateral ligament (UCL) starts to thicken and become more pliable, which means it’s less stiff. Yes, you guessed it—working on gaining greater passive external rotation range of motion while the ligament becomes more pliable is not good. You are taking the catapult back further, and the hinges are not as strong. Ultimately, if you are not checking strength levels, you are making the arm like Gumby and less like Popeye (might be outdated for some of you with this analogy).
The bottom line is that you are in trouble if you are not looking at both strength and only length.
Read ISSUES WITH PASSIVE RANGE OF MOTION TESTING to learn more about the problems faced by relying only on passive ROM testing.