Strength in Numbers #147
The tables have turned.
Throwing fast may be a thing of the past, at least in the sense of trying to deliver the baseball at maximum intensity. However, I am still not convinced that if you throw a high-octane fastball, you are going to receive an automatic doctor’s note to have your arm surgically repaired.
If that’s the case, Nolan Ryan wouldn’t exist.
Yes, the percentage of MLB pitchers having TJ surgery has increased, but don’t you think it would be way higher?
The way we are talking now is that if you throw over 95 mph, your ulnar collateral ligament (UCL), that little connective tissue bridge between your forearm and your upper arm, should be a ticking time bomb waiting to explode.
But that is way further from the truth.
THE MISINFORMED
I remember reading an alarming research paper in 2012, more than ten years ago, and Tommy John Surgery was still rampant and a problem then.
In the research article “Public Perceptions of Tommy John Surgery,” Dr. Ahmad, a long-time surgeon in professional baseball, interviewed many people to obtain their opinions on the matter.
Here are the results:
Thirty percent of coaches, 37% of parents, 51% of high school athletes, and 26% of collegiate athletes believed Tommy John surgery should be performed on players without elbow injury to enhance performance.
Risk Factors: Thirty-one percent of coaches, 28% of players, and 25% of parents did not believe the number of pitches thrown to be a risk factor, and 38% of coaches, 29% of players, and 25% of parents did not relate pitch type (e.g., curve balls) with risk of injury.
Benefits: Many players (28%) and coaches (20%) believed performance would be enhanced beyond their pre-injury level.
Return to Play: Individuals underestimated the time required to return to competition. 24% percent of players, 20% of coaches, and 44% of parents believed that return would occur in < 9 months.
Now, we need to have common sense here. Surgically operating on elbows as a preventative solution seems absurd.
Still, a good percentage of people think Tommy John Surgery is elective and should be done because of the mentality that “everyone is going to need it anyway.”
This study was conducted long before the pitch clock, the sticky stuff, and any talk of the velocity bug. Um, Houston, we’ve had a problem for a while.
ENTER THE VELOCITY-TORQUE RELATIONSHIP
Without going into a ton of detail, only one study has ever connected joint loading to injury and fastball velocity to injury. That study was done on 23 pitchers using 2D video footage.
It is archaic by today’s standards, but there is tremendous merit to the research, as it did look at in-game biomechanical data that was hand digitalized and that is unique even by today’s standards in motion capture.
In the investigation, some individuals in both the injured and non-injured groups had identical velocities, meaning you could throw 85 mph and still have TJ surgery. What is even more interesting is that the velocities recorded in the study for the injured group, featuring MLB-affiliated pitchers, fell short of today’s best high schoolers.
The interesting fact that was not truly emphasized was that career length was longer in players who required TJ surgery.
That glaring confounding variable makes this whole story anything short of suspicious, as they simply threw more pitches. If you want to know more about the study I am talking about, please read about it here.
Since the extent of risk associated with high-velocity deliveries is not known, why do some pitchers who throw slow and some who throw fast still have TJ surgery?
Well…that, in part, is a matter of the individualized velocity-torque relationship both between individuals and within themselves.
Research has uncovered almost no correlation between throwing at high velocity and joint loading. We could have three pitchers throwing all that at the same velocity—let’s give it a number like 100 mph—and all three will have different elbow torque imparted on the inner elbow, which, in part, must be stabilized by the UCL.
However, within pitchers, as velocity climbs, elbow torque does increase as well—yet that doesn’t mean it is uniform between players. On average, 1 MPH = 1 UNIT INCREASE in elbow joint loading. However, there are exceptions to the rule.
Some pitchers could throw four pitches at four different velocities (97mph, 98mph, 99 mph, and 100mph), and the joint loading could be minimal, if any, detectable difference.
On the flip side, a player who throws four pitches from 82-85 mph could have an extremely sharp rise in elbow torque, meaning that the velocity-torque relationship has a sharp slope and presents a greater injury risk if the throwing arm is weak.
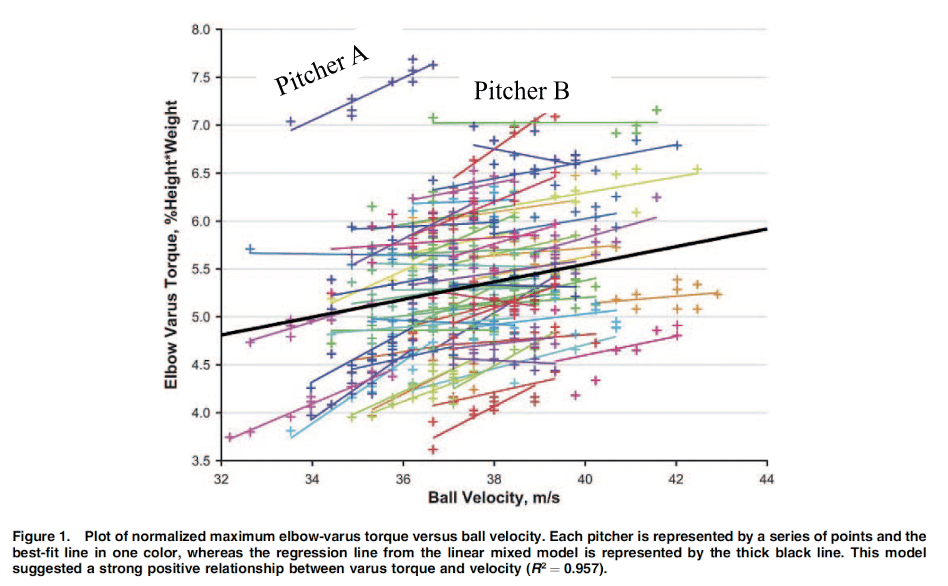
Take one of the first research articles ever published on the velocity-torque relationship by Dr. Jon Slowik and the research group at ASMI.
They looked at velocity-torque relationships between pitchers and within.
There was no correlation between pitchers and elbow varus torque, meaning that you could throw at high velocity with less torque on the inner elbow than pitchers who may throw at significantly slower velocities with higher torque, and this refutes the idea that all pitchers that throw hard are exposed to greater injury risk.
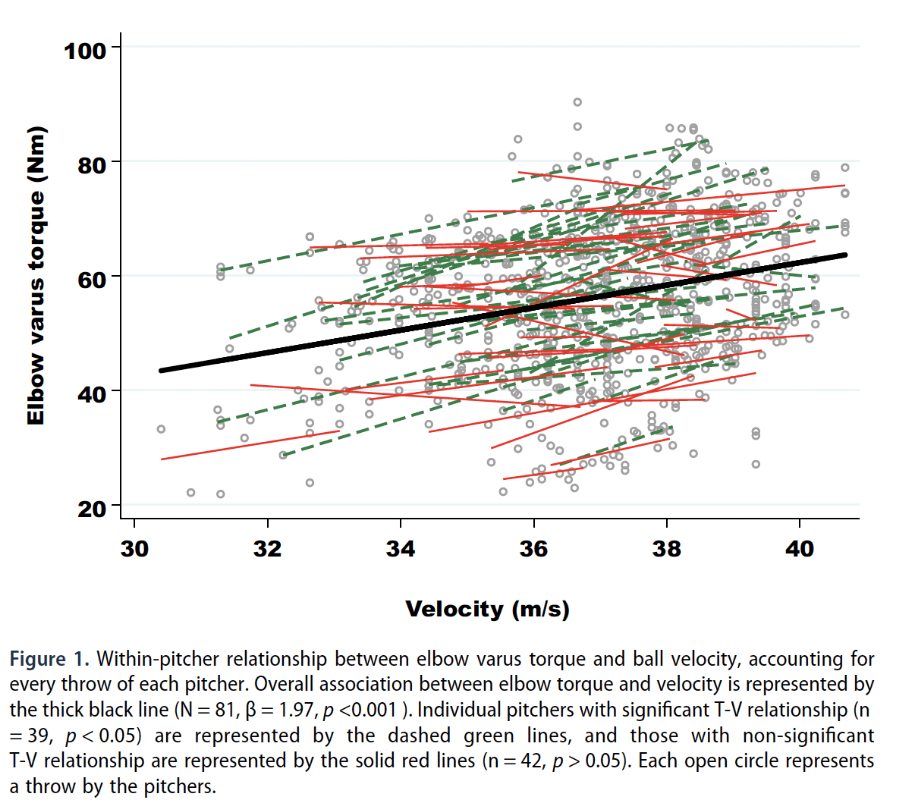
Another study on collegiate pitchers discovered a similar trend with the lowered predictive ability to actualize joint loading from throwing velocity.
Like the previous research above, comparative analyses between pitchers had low predictability, so throwing out a velocity number, like 100mph, doesn’t seem to have a consensus that all pitchers have the same joint loading, as some may have lower elbow torque values compared to pitchers who throw 10 mph slower.
SO NOW THAT YOU ARE ROYALLY CONFUSED – HOW DOES VELOCITY CAUSE INJURIES?
The short answer is that it doesn’t cause injuries. It’s an association.
You can throw hard, you can throw soft, and you are still at risk of TJ surgery.
You can have soft-throwing pitchers with high elbow torque and a sharp velocity-torque association, hard-throwing pitchers with low elbow torque, and some with a downward velocity-torque association, meaning torque reduces as they throw harder.
Your issue is that you will not know which pitchers have a sharp, flat, or negative velocity-torque association unless you perform a 3D motion capture study on every one of them and have them throw at incremental velocities to obtain the most accurate predictive model.
Similarly, the velocity-torque relationship can change with throwing arm fatigue, which causes compensations.
So, what is the best defense? Stick to the averages…
1 MPH = 1 UNIT of ELBOW VARUS TORQUE.
That means if your player gains 10 MPH, each throw could be considered to have increased loading by a factor of 10. Multiply that by 1000s of throws in a season, and it’s a problem only if you cannot absorb it.
In the last Strength in Numbers, you learned about the Stress-Shielding Ratio.
Attributing TJ surgery to velocity on its own is convoluted, but it is undeniable that throwing arm weakness is a problem.
But don’t worry! We’ve got you covered if you are gaining velocity and losing strength. Just look at the Strength-Velocity Ratio in the app and make sure it is blue and above 1.6.
In simple terms, if you throw 100 mph, you better have 160 lbs of throwing arm strength, or you are overreliant on stretch-loading, which may create greater tension on the hinge of the catapult, which is the UCL.
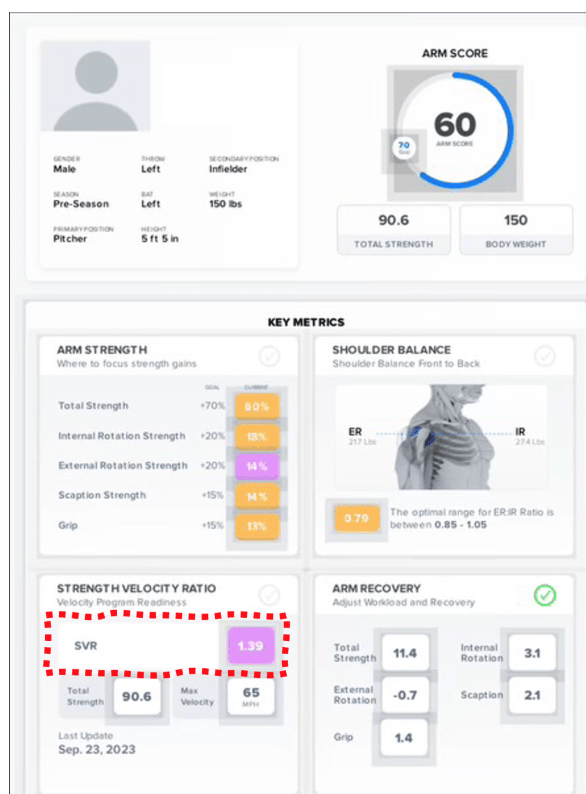
As a basic rule, if you are under 1.6, have low relative throwing arm strength to your body weight, an unbalanced arm, or one that fatigues and doesn’t recover, you have work to do whether your pitcher has a cannon or a squirt gun.
The bottom line is that stronger arms are harder to kill, no matter how fast they move.
Strength Matters Most,
Ryan
Ryan@armcare.com