Strength in Numbers #151
To date, the performance of our platform and product has been exceptional in preventing throwing arm injuries.
The national average is that 5% of all pitchers yearly will have throwing arm surgery (ref). There are millions of players taking the mound in the country, and only three using ArmCare have required surgery since 2020.
Recently, a parent reached out about a non-surgical injury his son had for the medial elbow. His son had been using our product, and as someone who is a scientist, I like to do science stuff.
First off, I am relieved that his arm strength prevented a surgical case, but nonetheless, this situation requires an autopsy, as I was burning to know how this risk was undetected.
Medial elbow injuries are my thing. I have spent 17 years studying Tommy John injuries, how to prevent them, their current epidemiology, return-to-performance rates, what to do across each stage of the injury, the precursors, contributing factors, and how to add durability to players while making sound monitoring decisions.
That said, there’s so much to learn because a UCL tear is neither bad luck nor a ticking time bomb for a pitcher.
There’s a reason for all of them. There are no flukes.
The best prevention is preventing the first injury. The research is a little inconsistent, but at the pro level, about a quarter of pitchers who have a forearm strain will have ulnar collateral ligament reconstruction.
WHY YOU NEED TO STICK TO THE DATA
Making program adjustments is hard for most players, especially among the players I advise, who are primarily high-round college players and pros. All of them are generally “team guys” and highly motivated.
Dialing down the throttle is not in their DNA, especially with draft opportunities and money on the line. They push through pain signals, sometimes alerts, and we scale.
It is definitely hard to tell an athlete who feels no discomfort or pain to skip a start, take a week off, recover the arm, and rebuild strength and shoulder balance.
Most of my athletes have had surgeries, some multiple, and I always say that the pain of sacrifice is so critical as the pain of disappointment is a true possibility.
They understand this concept. Either way, there will be pain, but the greater majority who have never gone through 18 months of disappointment from a complete reconstruction ignore the signs.
I will walk you through an actual situation where I dove deep. Injuries of any kind burn me up, but when you have a data-led option to assess your throwing arm and feed it customized training, that dials me in like a predator about to devour its prey.
If they had only seen things if the athlete had only communicated, they could have acted, for if they had, I guarantee the arm would have been more resilient. This injury involved velocity enhancement training at one stage but did not follow our ThrowFuzz Checklist, an essential framework to minimize risk and maximize performance.
The Case
Here is the email we received about this player…
Hi. He was pitching in a game, first 2 innings were great. 3rd inning it looked like something was wrong cause he was missing glove side the whole time. He did not say anything about pain until a couple of weeks later when he was put down to JV and pitched and continued to throw out and velo was off. He went to the trainer who said his forearm flexers were tight and everything would be ok after 2 weeks rest. I took him to PT and they said his UCL was very strained because his forearm muscles were very tight. They did therapy and dry needling, and he said that it felt like they deflated a balloon.
2) We have been kind of taking it slow, we are out of high school ball and threw his first live BP this week. We will get back on it as soon as we can
3) I think he is recovered but I’m assuming he is scared to throw hard cause of the dreaded surgery we don’t speak of (TJ)
In reading this text, here are some very important messages to take to heart:
- NEVER THROW THROUGH PAIN – Pain is an indicator that something is inflamed. This generally comes with a lack of stress-shielding the muscle’s ability to protect the UCL. Unfortunately, this athlete ignored pain and kept throwing through it until it was bad enough to shut him down.
- TIGHTNESS IS WEAKNESS – Getting back to stress-shielding, when the arm has loss of force absorption (weak collagen fibers, lack of neurological responsiveness to contract, nutritional deficiencies, or reduced circulation), the forearm will tighten. It’s trying to make a cast to protect the ligament. It’s telling you, “Hey dude, stop throwing NOW. My grip strength has weakened in some manner”. Oftentimes, athletes try to stretch through it, but it definitely comes with pain and soreness as the inner elbow is fighting to stay away from stress – force applied to cross-section tissues.
- NEVER RESUME A THROWING PROGRAM WITHOUT OUR ALGORITHM FOR RETURN – The majority of baseball players everywhere are going through rehabilitation programs without objectively testing strength. I am not saying that clinical feel has no relevance, but when it comes to high-speed motion, a conservative or surgical injury, you do not release a lion into the wild without its claws. The claws are a robust arm. Often, athletes speed through an interval throwing program, some designed in 1985, and then go out and try to pitch their daily max only to have a consecutive (same injury) or subsequent injury (a new injury) to their throwing arm. Incomplete rehabilitation is 100% reality, and what scares the $HIT out of me is that physical therapists and athletic trainers tend to de-prioritize the strength of the arm and focus more on a range of motion and absence of pain (ref). The neurological condition of the throwing is unknown unless you maximally activate it and test it regularly. It is an act of the Lord that we reached out to this parent, as their son made huge increases in their ArmScore, which is a good thing that paralleled velocity enhancement but needed more context into the alerts, and we emphasized that the play.
THE AUTOPSY: THE FRESH EXAM
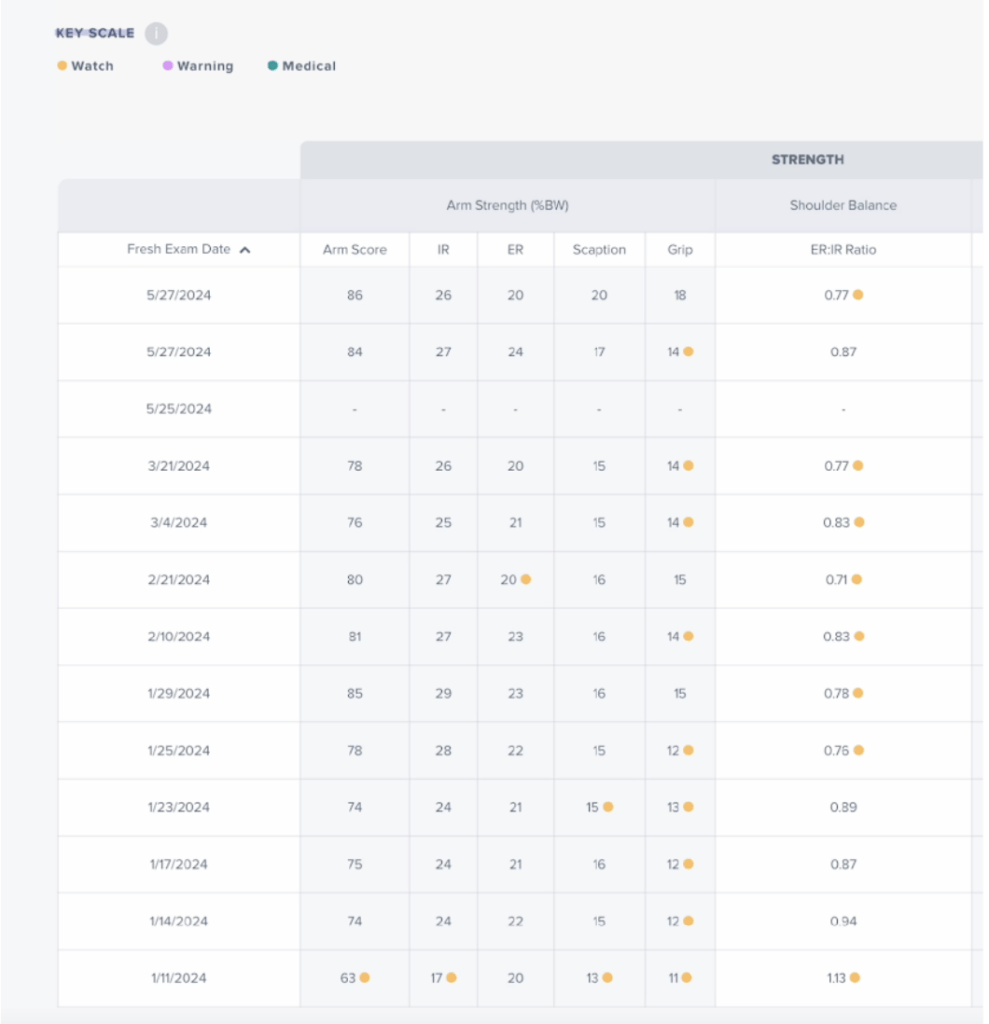
In summation, it is easy to see an alert on each test. That means we need to fix the problem. Lower the throttle on throwing intensity and dial up the training. These warnings are related to many factors, and we need to determine whether it’s weakness, fatigue, or poor recovery. Still, it’s obvious that this athlete had weak grip strength that could have led to significant microdamage and loss of stress-shielding until the pain was overbearing, not to mention that the shoulder has been imbalanced for much of the testing that had gone on.
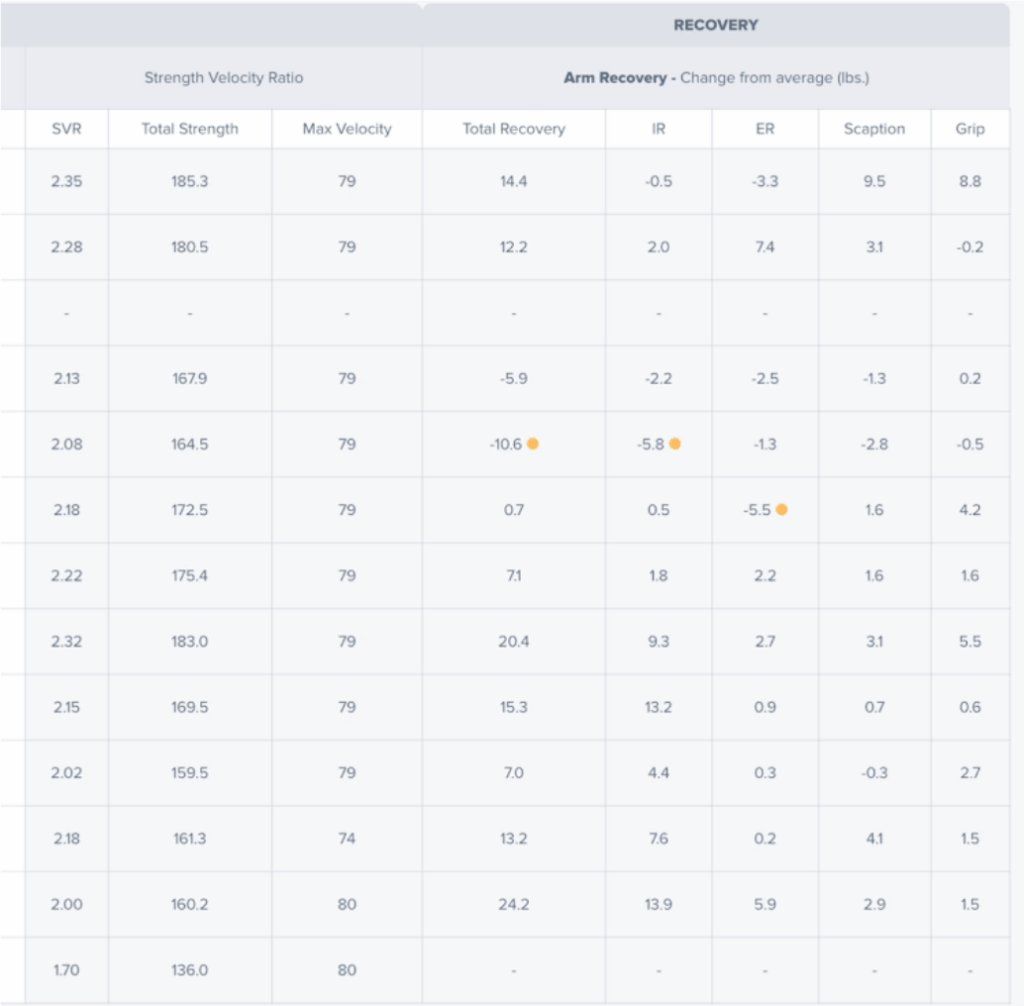
When it comes to the SVR, everything checked out. This athlete has a very high strength to velocity (LBS/MPH). This tells us that he relies on muscle force rather than passive stretching to deliver the baseball and narrows in that this was more a muscular problem as a primary contributor. Athletes with scores lower than 1.6 have high-level mobility and stretching capacity. For the lack of force in producing velocity, they make up for it by stretching passive stabilizers like ligaments.
You will also notice that this athlete had poor recovery, only two tests before the injury shutdown. If you add up all the strength lost, it totaled over 20 lbs. Think about that, pick up a 20lbs dumbbell in your hands. Imagine that kind of strength leaving the throwing arm and then going out and trying to let it eat. Intuitively, there is a recovery problem that leads to the presentation of forearm tightness. His flexor pronator mass loses elasticity (force absorption when lengthened, known as eccentric contraction) as it is literally trying to build a human cast around the origin and insertion of the ulnar collateral ligament. Suffice it to say that athletes need to review all their data, hit all the buttons on the app, and take everything seriously.
THE AUTOPSY: THE POST EXAM
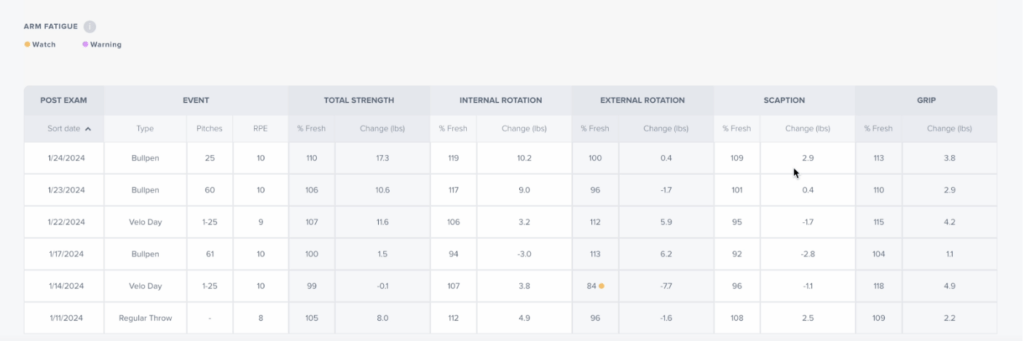
Here’s my issue. The post-exam looked solid going into January. However, the numbers are so high that it tells me how neurologically this athlete could be wired. Remember that his injury happened early in the spring season, and this athlete stopped testing.
There is no doubt in my mind that throwing arm fatigue played a part in this, and it is also alarming that the athlete was in a velocity enhancement program when his grip strength and shoulder balance were alert. Again, please follow the ThrowFuzz Checklist, as this was not the direction to take. Microdamage can be cumulative, and it’s possible that he encouraged more damage during this period, which influenced his arm health in the spring.
The absence of ArmCare testing is a significant problem for me, and it may not be the athlete, but the coaching staff may not want athletes to test in the season, which is a huge problem and has happened at least with one of the athletes who I now consult for after his head coach said nothing extra in-season and that can come with reduced strength training all around.
This is what happened in the season. The athlete encouraged more significant fatigue when the throwing arm was weak and imbalanced. The fatigue had dropped out the strength of the elbow region. Each fiber that cannot absorb increases the stress applied to the ligament. The micro-injuries intensify in season.
Every time out, you are throwing at maximum capacity, and the athlete cannot know that his arm is fatigued. The arm did everything to tighten the area with the most responsive fibers it had to shield stress, but it was ineffective, and more shielding loss occurred; thankfully, the pain was intense enough for this athlete to stop throwing, seek treatment, and avoid surgery.

As I mentioned above, there’s a reason for all injuries. We have identified some critical pieces of information to help this athlete. We are very grateful for our customers’ messages when a problem arises, as we can review the data and present the de-identified information to our audience.
We want to keep this player safe, and in doing so, we are keeping you safe. He is the hero of the story. We are only the guides.
Injuries show us how to improve, and as I always say, injuries are not breakdowns; they are BREAKTHROUGHS. This athlete is now more equipped to protect his arm and advance his durability.
Here are some important take-home messages:
- NEVER THROW THROUGH PAIN. DON’T TEST YOUR ARM, AND DON’T DECIDE TO KEEP THROWING IF ONLY A FEW THROWS BOTHER YOUR ARM AND THEN IT FEELS GOOD AND COMES BACK (TRANSIENT ARM PAIN). ARM PAIN IS ARM PAIN, AND I HIGHLY RECOMMEND THIS COURSE ON HOW TO ELIMINATE PAIN AND SORENESS.
- DO NOT MISS TESTS. TEST BEFORE AND AFTER BEING ON A MOUND OR HIGH-INTENSITY THROWING DAYS, LIKE BULLPENS OR PULLDOWNS. DO THIS ALL YEAR LONG. DON’T STOP IN WHEN IN SEASON.
- MEET OUR THROWFUZZ CHECKLIST. YOU CAN NOT PARTICIPATE VELOCITY ENHANCEMENT WHEN YOU HAVE ALERTS. STOP AND FIX THEM.
- THE PAIN OF SACRIFICE NEEDS WIN OVER THE PAIN OF DISAPPOINTMENT. BE SELFISH IN YOUR SELF-CARE. YOU NEED TO HIT THE GAS, TAKE YOUR FOOT OFF THE PEDAL, AND PUMP THE BRAKES ACCORDING TO YOUR ARMCARE METRICS. YOUR TEAM WILL APPRECIATE YOU MORE WORKING ON YOUR ARM RATHER THAN NOT PITCHING FOR THEM IN 18 MONTHS.
- LOOK INTO SPORTS PSYCHOLOGISTS IF YOUR ATHLETE IS SHOWING SIGNS OF HEALTH ANXIETY OR KINESIOPHOBIA – STOP THE BRAIN CYCLE THAT “MY ARM IS GOING TO BLOW UP”, OR “I CANNOT THROW HARD ANYMORE, I AM AFRAID”, “OR MY CAREER IS OVER IF I GET HURT.” IF YOU SENSE YOUR ATHLETE IS HAVING ISSUES THAT ARE ROOTED IN WHAT I CALL THINKING ERRORS, PLEASE EMAIL ME, AS THE MIND WILL ALWAYS WIN AGAINST THE BODY.
AND NEVER EVER FORGET – STRENGTH MATTERS MOST.
PRIORITIZE IT. VISUALIZE IT. ANALYZE IT. FORTIFY IT.
Ryan
Ryan@armcare.com