Strength in Numbers #146
Read Part 1 here and Part 2 here.
This article has not been fun to write. Having to to discuss where I felt short for not just a player but a friend to over 30,000 people has been difficult.
It is dense with evidence-based practice and a practice-based evidence approach to attacking Tejay’s problem, which is also a problem for every hard-throwing baseball player. It’s taken three weeks to write this, and I would appreciate 5-6 minutes of your time.
Throughout his injury, until he had his surgery and set his sights on a comeback, Tejay took a lot of heat on social media about what happened to him. That infuriated me, as he, like any athlete, was already going through hell, and people on the periphery criticized him, and then it was directed at me.
“He should fire you. You should have used my product. Your objective data is meaningless without my skilled hands and my 50-point checklist. Athletes should go into clinics and see real sports medicine specialists, not some egg-head scientist who pretends to be a strength and coordination specialist. Your ArmCare device is masquerading around as a Velo Program getting players hurt.” The list goes on and on.
For any athlete who has experienced injury, learn from your learner. Tejay is one of the most open athletes in the game and is most willing to process and apply research.
He worked with great people who covered all the blind spots with the Reds. As a leader in the coaching world, he also understands what is going on at lower levels of play—look below.
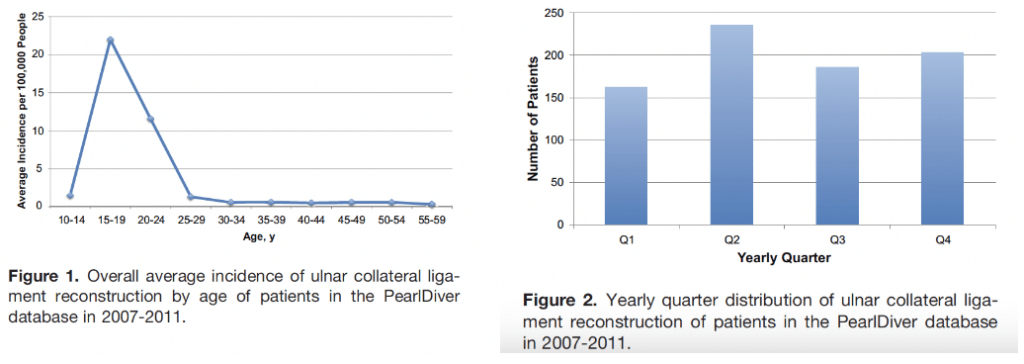
Erickson, Brandon J., et al. “United States trends in medial ulnar collateral ligament reconstruction: a retrospective review of a large private-payer database from 2007 to 2011.” Orthopaedic Journal of Sports Medicine 3.7_suppl2 (2015): 2325967115S00092.
You get real, real fast, about many things, and then the client relationship turns into a friendship. When they go through something bad, you do, too.
I am facing the chin music, pointing fingers at myself, and, with the help of Tejay, pointing you in the right direction. My mother used to say, “No pressure. No diamonds.” With the buzz of what’s happening around the pitch clock, there’s plenty of pressure in the game that can do wonders if we can start focusing on the throwing arm and eliminating distractions.
THE SENSITIVITY OF REVISIONS
The number of primary surgeries worldwide is growing. The average UCL reconstruction lasts less than 3.5 years.
It’s essential that we set our sights on how to prevent revision surgeries in addition to avoiding surgery in the first place. Roughly 85% of pitchers come back from the first surgery, and after the second, that number can be cut in half, and a consensus has not been reached and could be less.
In my academic career, I have participated in a couple of really interesting studies, but one that has taken the cake was the work performed at Waseda University in Japan under one of the greatest biomechanists I have ever encountered, Dr. Toshimasa Yanai.
This man has done more innovative things than anyone I know from a technology integration perspective. He has written his own software to track scapulohumeral movement and global 3D movement. He was the first to study ground reaction force data in the mound by soil-infused force plates so that cleats could be worn. He is also the modern forefather of elbow varus torque strength testing and the shielding stress quotient needed to protect the elbow.
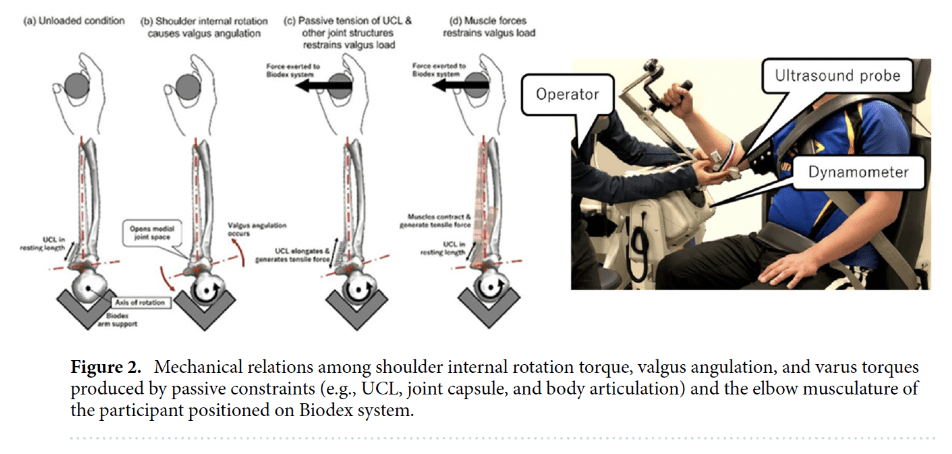
We published a special article in Scientific Reports for Nature, a well-known science publication. It was an interesting study with some critical implications on the power of dynamic elbow strength in pitchers who have had a prior UCL repair.
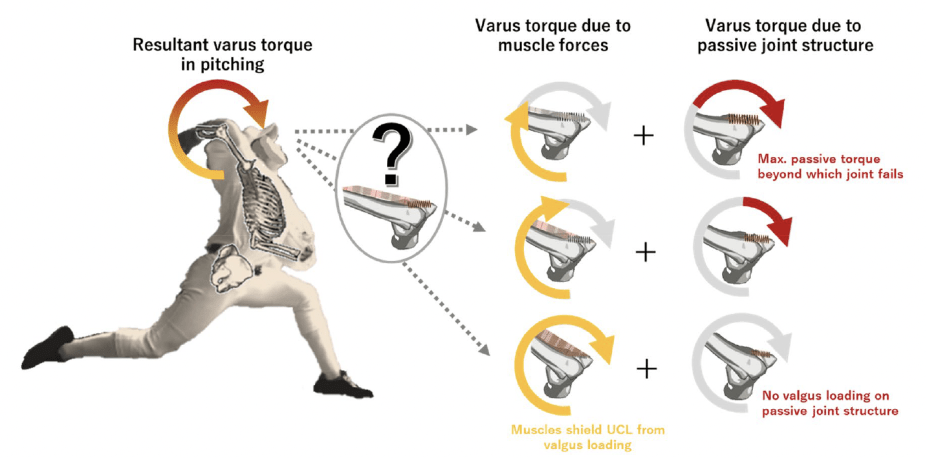
Note that as the arm lays back, the effectiveness of the dynamic stabilizers (yellow shaded region of the elbow) changes in the length-tension relationship, while passive restraints such as the UCL increase the risk of overexposure to loading. In a nutshell, muscular strength from the flexor-pronator mass needs to be optimized to protect the UCL and offload tension as the forearm moves from max layback toward acceleration to ball release.
Yanai, T., Onuma, K., Crotin, R. L., & Monda, D. (2023). A novel method intersecting three-dimensional motion capture and medial elbow strength dynamometry to assess elbow injury risk in baseball pitchers. Scientific reports, 13(1), 12253
This study taught me the real complications associated with a UCL that has already been repaired, and you should take note of this right now. You all know someone who has had TJ surgery, so this is important to grasp.
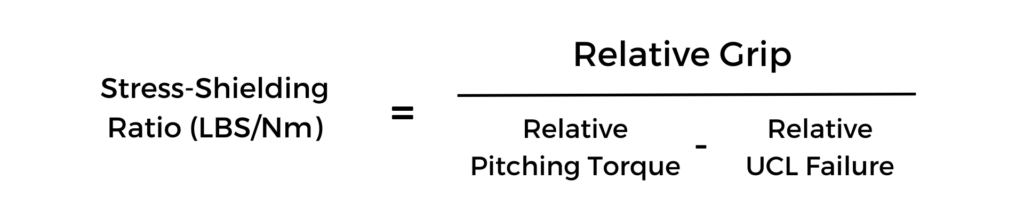
BEHOLD THE ELBOW VARUS TORQUE STRESS-SHIELDING FORMULA:
In general, a 90-mph fastball imparts roughly 100 Nm of valgus loading to be absorbed by the dynamic stabilizers of the elbow. However, what is not known to the public is that the UCL will fail at 35 Nm, which means that the muscles need to shield the ligament, as every single throw would blow it apart. Now, take the already surgically repaired ligament; the failure point can be as low as 20 Nm. Just think of how strong the dynamic stabilizers of the inner elbow must be to shield the athlete’s ligament a second time.

This stress-shielding formula accounts for the 3D torque required to withstand the valgus loading measured during pitching for the elbow, the UCL failure point, and the elbow varus torque strength from a Biodex, the most sophisticated strength tool ever made that can generally only be found in laboratories like this one and one that we have at Louisiana Tech in the Human Performance Labs overseen by Dr. David Szymanski where I am a research associate. The %MVIVSmin indicates the theoretical intensity of muscular contractile output required to prevent the UCL from blowing apart.
On a fastball alone, the elbow musculature had to produce a varus torque to completely unload the UCL as high as 97% of its maximum varus torque strength in every pitch. When accounting for the theoretical load taken up by the UCL in pitching and the minimum strength requirements based on the formula above, muscles need to contract at their highest for fastballs and sliders at about 60-65% of the elbow varus torque strength maximum to shield the ligament that does contribute to elbow stability. If the athlete has an intact UCL that has never been surgically repaired, the maximum strength required decreases to roughly 50% as the ligament has a higher failure point when intact.
THE ELBOW VARUS TORQUE STRESS-SHIELDING FORMULA MORE SIMPLIFIED:
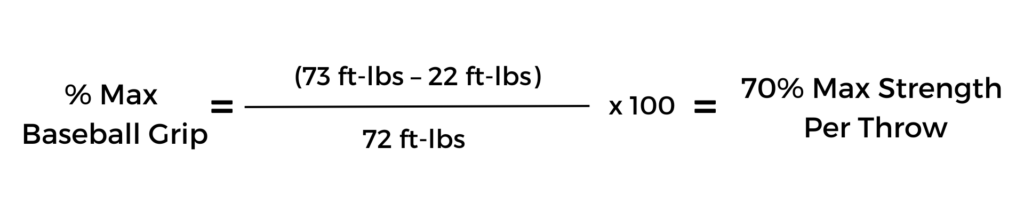
Okay – so now let’s put it in real terms using pounds and ft-lbs with the baseball grip pinch strength test.
Let’s say an athlete with an intact ligament has a total pinch grip strength of 72 lbs. Then we plug in the varus torque imparted by the elbow stabilizers (i.e., the UCL) during pitching to combat the valgus loading for a 90-mph fastball, which is, on average, 73 ft-lbs. In this case, we’ll say the UCL can handle 22 ft-lbs. Let’s also say that athletes in these case studies are 6 feet with a forearm length of 1 foot.
Take the same pitcher who has had revision surgery, and let’s plug everything in. The only difference is that the UCL can handle less torque, which decreases the ft-lbs to 18.
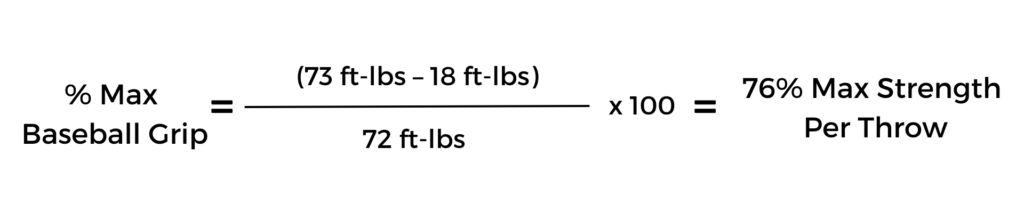
This example shows that the impact of fatigue may be more prevalent in a player with a UCL reconstruction because greater percentages of maximum strength is required to offload it. The other side of the coin is an increased need to improve their maximum grip strength to lower the strength needed to protect the ligament.
Okay, let’s take a high school kid with low grip strength who has not had a prior TJ surgery and raised his velocity from 10 mph to 90 mph without a change in grip strength. This athlete has 31 ft-lbs of absolute grip strength.
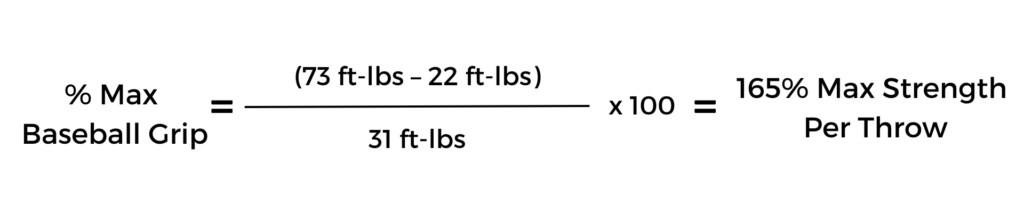
Obviously, with the high school athlete, the auxiliary muscles of the shoulder must be highly recruited and balanced to lower the percentage of maximum strength required to shield the ligament. You can see how weak arms that throw hard are in trouble.
MORE SIMPLY–THE STRESS-SHIELDING RATIO
To make the calculation easier, you could also evaluate stress-shielding capacity by looking at normalized data to compare athletes using relative grip strength and a 90-mph average relative fastball torque of 100 Nm.
STRESS-SHIELDING RATIO Examples
Athlete 1 (6 feet, 200 lbs, LHP)
- Relative Pitching Torque Measured by 3D = 6.2% body weight * height
- UCL Torque = 1.85% body weight * height
- Grip Strength Relative Max = 15% body weight
Athlete 1 Stress Shielding Ratio = 15/ (6.2-1.85) = 3.45x
This means that the relative grip strength of Athlete 1 is 3.45x the failure point of the UCL
Now, let’s say Athlete 1 has had TJ surgery (UCLR means UCL reconstruction) and now throws 95 mph, increasing relative elbow varus torque by 0.27% and reducing the relative UCL failure point.
- Relative Pitching Torque Measured in 3D = 6.47% body weight * height
- UCLR Torque = 1.56% body weight * height
- Grip Strength Relative Max = 15% body weight
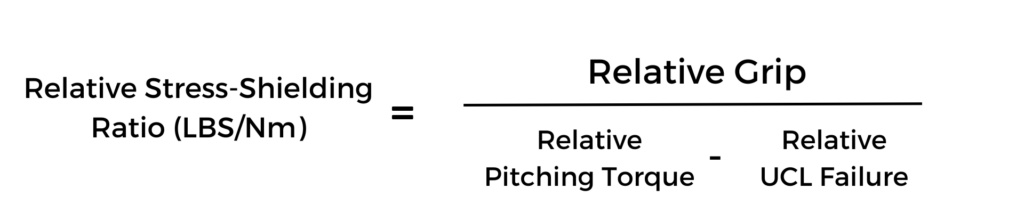
Athlete 1 Relative Stress-Shielding Ratio = 15/(6.47-1.56) = 3.05
The 3.05x factor means that Athlete 1 has lower stress shielding ability because his forearm strength to protect the UCL is relatively weaker compared to the torque applied by pitching.
I hope you are catching my drift. The secondary revision needs a lot more strength, with approximately a 12% loss in stress shielding due to the ligament’s inherent weakness and increased pitching torque from velocity enhancement.
This brings me to where I see a flaw in what I had taught and preached.
This science confirms that our approach with ArmCare.com needs more attention for our hardest-throwing pitchers—the relievers, especially those who throw 100-mph relievers and have had two revision surgeries.
MISSED OBSERVATIONS
In our courses, through simulations and personal experience serving athletes at the highest level, you generally catch a reliever in a recovered state every 72 hours to accurately capture maximum strength data and not over-test the arm. In prevention, especially for closers, you miss the possibility of going into a game for a third time with a tired and poorly recovered throwing arm. In the case of Tejay, he made his way back in 2023 and flourished in 2024, going back-to-back without any issues. We narrowed the gap to 48 hours, and I have since rethought that approach. It was not frequent enough.
With relievers reaching triple digits and average velocities above the MLB average, I recommend testing the throwing arm every 48 hours at minimum, and they will communicate if it’s too fatiguing, which I have not had that problem with my athletes.
However, if any athlete you have on your staff has had a primary UCL reconstruction, which I think now is 35% of MLB, I recommend you test the athlete within 24 hours of an appearance. You should not miss that time window as I have revealed above what a change in strength may be and have written the past two articles for you to learn about UCL prevention and occurrence. The athlete may not be in a recovered state, but the point is, especially if they are going back-to-back, identifying if they are recovered.
The scientist in me had become more of a realist when entering MLB. We did not have a Biodex, and we barely had any staff available to operate technology for our players. We did have success even with a homestand strength screen, no surgeries to our active roster for the two years, and individualized arm care programming and routine strength monitoring in place. It was rough on our staff and ourselves.
The other error that I cannot stress is the importance of manpower over computing power. My consulting business has grown very quickly, and when it comes to a player like Tejay, a team must be built around him, even though he is very self-sufficient. He runs the ArmCare platform with his entire performance company, which is at the forefront.
I remember how badly I needed people over technology when I was in a leadership role in MLB, but now the technology is in a player’s hand, and our world can truly be player-led and coach-informed. It also allows others to give players and teams a helping hand and lessen the burden and role strain from being stretched thin.
Can you imagine a world in which players can evaluate their arms and inform coaches and staff how to adjust throwing arms with objective data, help shape throwing plans and appearance schedules, and be dynamic with arm care training around the clock?
This world is now. With the emergence of pitching injuries, blaming a technical rule problem with the pitch clock does not solve the problem; it merely points out an association that impacts stress shielding. It’s time we looked more introspectively and understood that the issues we have been faced with today are observation problems.
There are more players today with revisions than ever before. When the student is ready, the teacher appears. We are ready, Tejay. Guide us to be heroes like you.
Yep..you guessed it…….STRENGTH MATTERS MOST.
Ryan
Ryan@armcare.com